
Stress Fractures: Part 2/4-Secondary Factors
When I see someone for physical therapy, one of the the things I want to know is their understanding of the situation. Without a doubt one of the most common answers is that something is wrong with their form. Makes total sense that this would be the thought for many when you consider how poor form as the sole cause of running related injuries is pushed by the media and social media influencers. In this follow up article, I want to explore that in the context of bone stress injuries (BSIs) as well as a couple other secondary contributing factors to their development; medications and baseline bone health.
Biomechanical Contribution
With research looking at the connection between biomechanics and injuries we have to first address a big limitation in much of this research. It is largely retrospective. That means we are looking at people who have already suffered the injury we are looking into. Therefore, we don’t know if what we are seeing existed prior to the injury, contributed to it, or if it is a result of the injury where the brain is trying to reorganize your bodies movement as a protective strategy.
Case in point is recent work by Whitney et al from 2025 showing an increased cross over gait pattern (feet cross midline when landing) and decreased abductor strength in those who had a femoral neck bone stress injury in their hip about 8 weeks prior. It would be easy to conclude that running with a cross over gait and having decreased abductor strength would be a risk factor. However, in the context of returning from a femoral neck stress fracture, the 8 week time frame is still quite early. In fact, I wouldn’t expect someone to be running and if they are, very minimally. Not to mention the time off they had initially. Just as it is easy to jump to the conclusion of these as risk factors, they may just as easily be non-existent should the study be repeated at a later date when further in the recovery process.
We also have some interesting probabilistic work from 2009 that looked at the probability of developing a tibial stress fracture based on stride length. (Edwards 2009) This work showed there was a significant, 3-6% reduction in the risk of developing a stress fracture when decreasing step length by 10% indicating strain magnitude on the bone is more important than the total number of loading cycles. However, predictive probability work is all based on math modeling and therefore, it does’t give us a clear lens into how this might play out in the real world.
Fast forward to 2021 and not only do we get to see this play out in real life, but also in a prospective study! (Kliethermis 2021) When taking baseline data of numerous gait variables of 54 collegiate runners and then observing them over 3 competitive seasons to see who suffered a BSI and who didn’t, many variables come out as significant players, but one in particular can influence the others and that is step rate. We know that step rate and stride length are intertwined variables effecting each other directly in that as stride length decreases, step rate has to increase and vice versa. Each step per minute increase in step rate resulted in a 5% risk reduction in developing a tibial BSI. While this is really important to keep in mind and consider, we can’t forget the bigger picture as not everyone needs to or should increase their step length. There are many things at play in the development of BSI and this is just one small piece.
For instance, this is really just looking at tibial bone loading rates and magnitude of force exerted onto the bone from impact (ground reaction force) and not including the force from muscles pulling on it. This is important to note because the muscle pull has a disproportionate contribution to the stress on the bone compared to impact in the overall force exerted onto it. (Matijevich 2019)

For those critically thinking minds who also remember my last article on this that centered around fueling and training being the primary causes of stress fractures, may have the following question. If these changes in gait characteristics increase load to the skeletal system, shouldn’t there be some level of adaptation over time that actually becomes protective rather than a risk factor? In theory, yes! As we stress bone more, the adaptation is greater resulting in a stronger bone that is more resistant to injury. That adaptation is quite slow though even under perfect conditions. If the fueling is inadequate or the training progresses too quickly, runners can still find themselves in trouble. In the event there are some biomechanical pieces stressing the bone(s) in question more, the training progression likely has to be even slower than we’d typically look at. There could also be other important factors that play a role as well.
Medication Contribution
Medications can play a pivotal role in our health and wellbeing, but sometimes we rob Peter to pay Paul. We utilize a medication to manage one diagnosis or symptom only for it to negatively effect another system or bodily tissue. Sometimes this trade off is worth it. Other times, it is talking to your physician about other potential options. Medications such as anticonvulsants, steroids, antidepressants, and antacids can have a negative effect on bone health. (Tenforde 2016, Chee 2014) There are very good reasons to be on these so if you have concerns about bone health please discuss this with your physician to ensure your prescription is the best one for you.
Architectural Contribution
The last secondary factor I would like to mention here is one that actually is established in our youth as the skeleton is growing and developing. Have you ever tried to break a stick for fun or at camp fire as a kid and come across one that you couldn’t quite break no matter how hard to tried? If I had to guess that one was either thicker or more dense than others you were able to break. Bone is much the same, the bigger and more dense we can get our bones, the stronger they become and less likely to fracture. Childhood seems to be the most opportune time to develop bigger and denser bones. You can certainly do this as an adult once physically mature, but it is much harder.
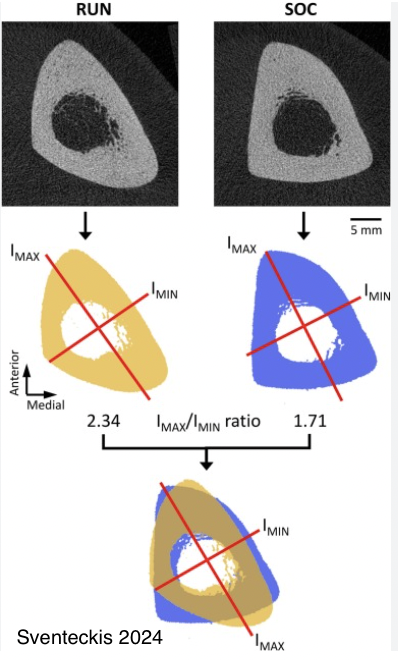
Bone likes short burst, high intensity loading that is multidirectional. Much like general play as a kid helps develop. Play is more difficult to quantify and track, but participation in ball sports is much easier. When looking at kids participating in ball sports compared to their more sedentary peers, we see significantly more developed bone structure resulting in stronger, more dense bones. Thus, this becomes a really strong protective strategy. When looking at youth soccer players compared to those who are more exclusively distance runners you see stark differences in their bone anatomy that directly relate to the strength and density of their bones, specifically the tibia (shin bone). (Sventeckis 2024) Additionally, it has been shown that soccer players have a reduced risk of fracture even 30 years later after playing. (Tveit 2015)
When we lack that history as many do, it doesn’t guarantee that you’ll develop a stress fracture. As I hope by this point you recognize there are always a multitude of factors. Don’t forget about the 2 biggest we wrote about in part 1. However, a lack of ball sports or considerable play in childhood does begin to increase the potential for a BSI should symptoms start to align with a typical BSI presentation. (Tenforde 2015, Milgram 2000, Fredericson 2005)
I plan to share additional information on this topic in 2 more upcoming articles on BSI’s in regards to how to best reduce risk and what recovery and rehab from a BSI should look like. If you need help navigating the intricacies of recovering from a BSI, please don’t hesitate to reach out to us or another trusted professional. I help runners recover from BSI’s and get back to training in Colorado Springs for in-person sessions and across the United States virtually. You can connect with us via phone at (719) 270-3155 or email at runmental@gmail.com. We are also active on Instagram where we frequently post educational material about running rehab and training.
References
Whitney K., Chanchi M., et al. Association Between Running Gait Biomechanics and Femoral Neck Bone Stress Injuries in Female Runners. PM&R. 2025;1‐11.
Edwards W, Taylor D, et al. Effects of Stride Length and Running Mileage on a Probabilistic Stress Fracture Model. Med Sci Sports Exerc. 2009 Dec;41(12):2177-84.
Kliethermis S. Stiffler-Joachim M., et al. Lower Step Rate is Associated with a Higher Risk of Bone Stress Injury: A Prospective Study of Collegiate Cross Country Runners. Br J Sports Med. 2021 May 14;55(15):851–856.
Matijevich E., Branscombe L., et al. Ground Reaction Force Metrics are not Strongly Correlated With Tibial Bone Load When Running Across Speeds and Slopes: Implications for Science, Sport and Wearable Tech. PLoS One. 2019 Jan 17;14(1):e0210000.
Tenforde A., Kraus E., et al. Bone Stress Injuries in Runners. Phys Med Rehabil Clin N Am. 2016 Feb;27(1):139-49
Chee C., Sellahewa L., et al. Inhaled Corticosteroids and Bone Health. Open Respir Med J. 2014 Jan 31;8:85–92
Sventeckis A., Surowiec R., et al. Cross-Sectional Size, Shape, and Sstimated Strength of the Tibia, Fibula and Second Metatarsal in Female Collegiate-Level Cross-Country Runners and Soccer Players. Bone. 2024 Nov:188:117233.
Tveit M., Rosengren B., et al. Exercise in Youth: High Bone Mass, Large Bone Size, and Low Fracture Risk in Old Age. Scand J Med Sci Sports. 2015 Aug;25(4):453-61.
Tenforde A., Sainani K., et al. Participation in Ball Sports May Represent a Prehabilitation Strategy to Prevent Future Stress Fractures and Promote Bone Health in Young Athletes. PM R. 2015 Feb;7(2):222-5.
Milgrom C., Simkin A., Using Bone's Adaptation Ability to Lower the Incidence of Stress Fractures. Am J Sports Med. 2000 Mar-Apr;28(2):245-51.
Fredericson M., Ngo J., et al. Effects of Ball Sports on Future Risk of Stress Fracture in Runners. Clin J Sport Med. 2005 May;15(3):136-41.